-
Lights, please
07/10/2016 at 22:58 • 0 commentsAfter a long and difficult time discovering the buccal ganglia, I recommend using a microscope with at least 6-8 Watt LED bulbs or else you will struggle to find the right area. The buccal ganglia is almost bikini-shaped as shown in the previous log from Ramakrishnan et al. 2014 and is seated directly behind the mouth. Best of luck!
-
A New Target
07/01/2016 at 02:07 • 0 commentsUpon reading a new paper, I have determined a new location for the electrode (when I get that point in the experiment): the esophageal trunk! Ramakrishnan et al. in 2014 studied the buccal A cluster (BAC) cells that fill up the buccal ganglia, 40 in each. These cells vary in location, size, and the cluster that they're in but essentially are responsible for telling different muscles to move, like opening the mouth or bringing the radula to the surface. All of these BACs have axonal projections through different nerves branching from the ganglia that we've talked about before: the lateral buccal neuron (LBN), the posterior buccal neuron (PBN), the esophageal trunks (ETs), and a few through the cerebro-buccal connective (CBC) that all then connect to different muscles. However, every one of these BAC projections goes through the esophageal trunks and none go through the ventro-buccal nerve. My plan was to attach the electrode to the trunk of the lateral and ventral buccal nerves, which is technically still okay, but only one nerve will be receiving signal. In the picture below from Ramakrishnan's paper, you can see that there are connections in every neuron except for the VBN with the lightest grey view.
![]()
HENCE I will be placing the electrode around one of the esophageal trunks for a *hopefully* stronger signal. Until I get to the point of electrode placement, I am continuing the search for the buccal ganglia.
-
On the Road to Postoperative Recovery
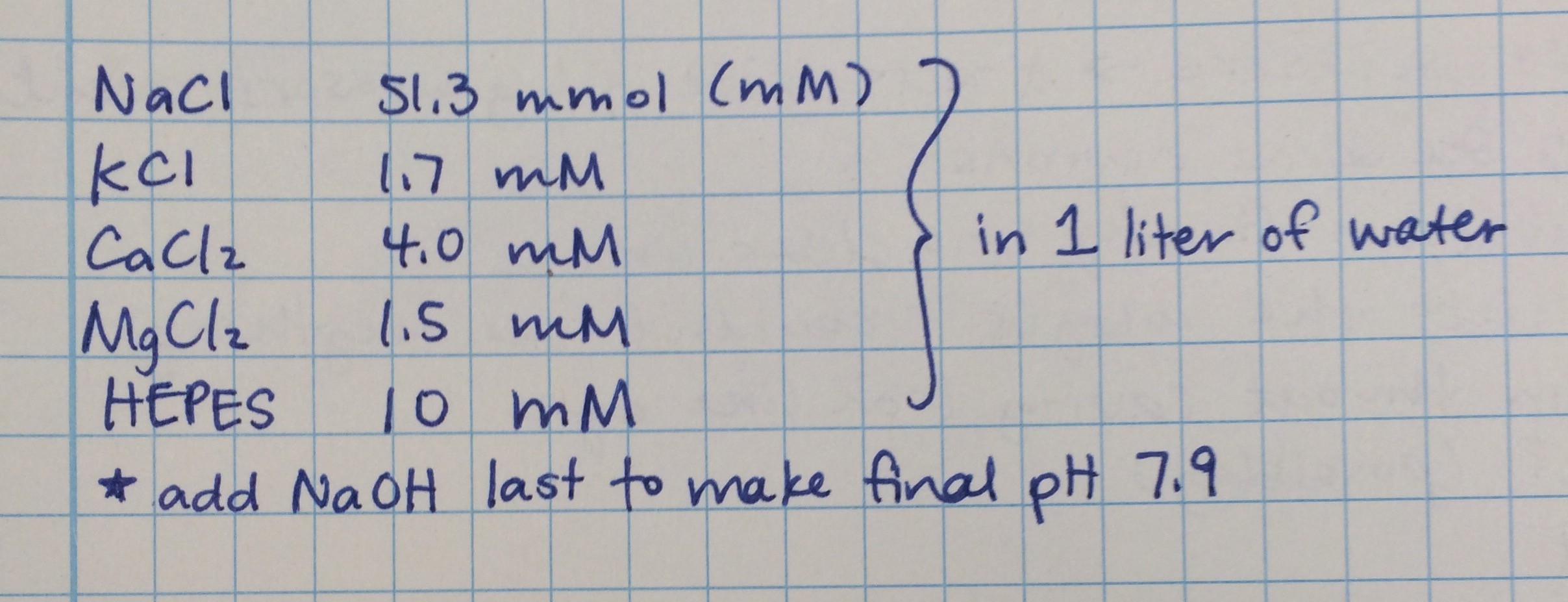
06/27/2016 at 20:36 • 0 commentsAfter going through surgery, usually humans can wake up from the anesthesia and function quite normally. Snails are not the same. After this procedure, they need to stay hydrated, but in something less anesthetic and more similar to their blood plasma. This is called a snail saline solution, or Ringer's solution. It's essentially 1 liter of water but with some very key components, like sodium chloride (NaCl) and a solution called HEPES. Below is the recommended concentration for each component which can be converted into grams of milliliters to add to the water. Sodium hydroxide (0.1 M NaOH) was added last in very small quantities to make sure the final pH of the solution was 7.9. This saline was provided by very kind and knowledgeable Lymnaea experts at Cornell. The snails can recover in this within 24 hours so place them in it for comfort and hopefully a speedy recovery!
![]()
-
Stop that snail!
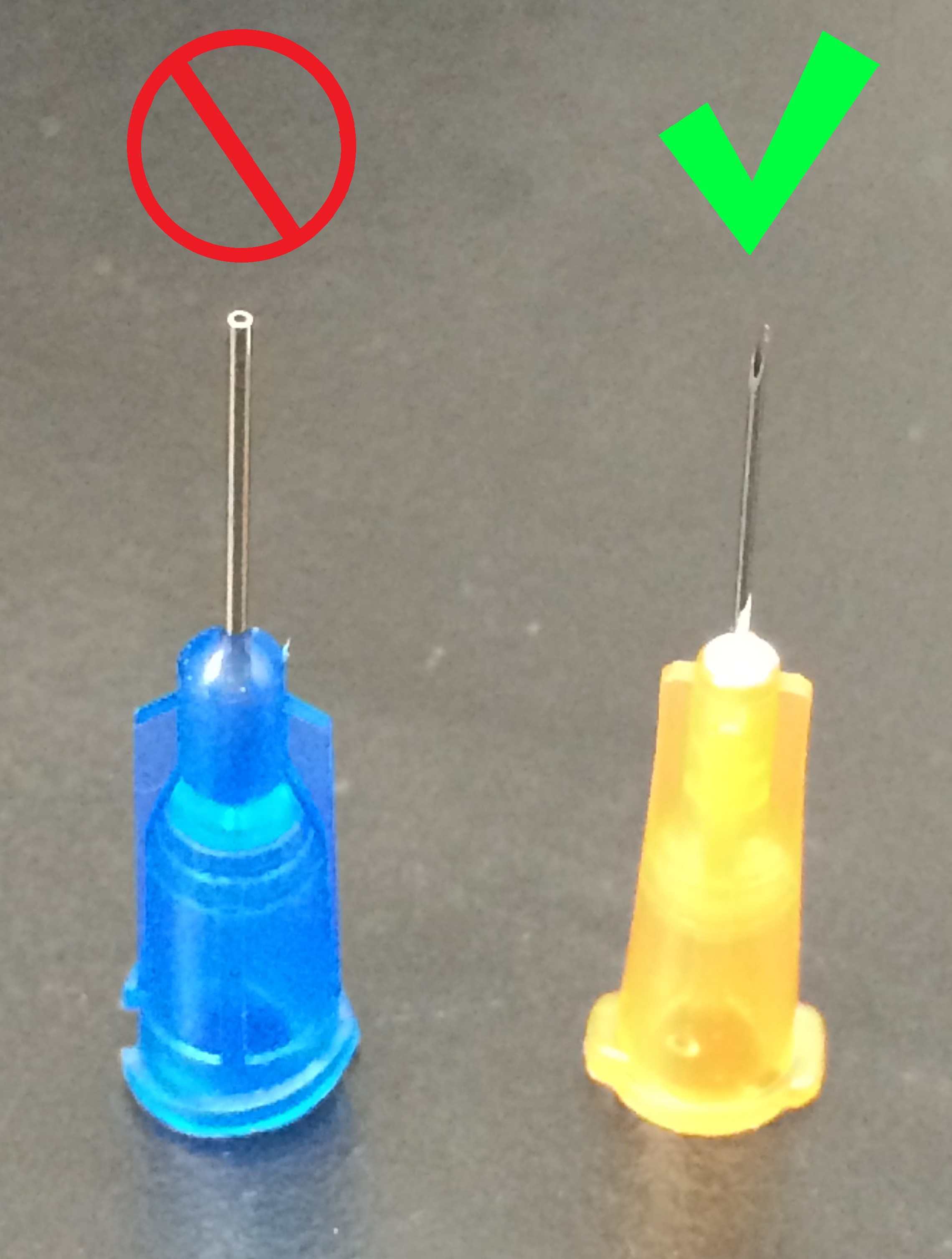
06/27/2016 at 18:54 • 0 commentsMore clearly explained, inject the snail before it hides behind its trap door anyway. For the past 2 weeks, I've had considerable trouble getting the needle into the snail to inject it with the anesthesia solution before the snail locked itself away in its trap door. It's actually a very fast and strong protection mechanism, considering it's a snail. I ordered needles off of Amazon that were wonderfully priced, however were not sharp enough to do the job. Even when trying to shave it down, it just didn't work. Your local CVS will have a needle for insulin injection so use that if you must. It has a beveled tip to the needle and a very nice 3 mL syringe for injection. Make sure you have these items before starting!!!
![]()
Zombie Snails: Mindless Methodical Movement
A study on central pattern generators (CPGs) that control eating behaviors in pond snails.